Cultural context of health is critical in responding to pandemics, new research shows: While populations’ access to health care is crucial to combating the spread of COVID-19, a team of Vanderbilt researchers has found that understanding the cultural context of health within a community is an equally significant factor—and can help leaders better prepare for future crises.
Monday, April 12, 2021
Saturday, August 1, 2020
Friday, July 31, 2020
WHO project on cultural contexts of health and well-being adopted in U.S.

WHO/Europe is pleased to announce that the cultural contexts of health and well-being (CCH) project, which it pioneered and established, will now also be rolled out in the United States of America.
Vanderbilt University will lead the United States-based CCH programme. This initiative has been made possible by support from the Robert Wood Johnson Foundation, which has provided a 3-year grant totalling US$ 600 000.
“Our cultural beliefs shape the way we think about health,” said Karabi Acharya, Director of the Robert Wood Johnson Foundation. “We draw from the experiences of countries around the world that bring the relationship between culture and health into sharper focus. Leveraging that global learning, this project will explore culture’s impact on our overall health and well-being in the United States.”
Nils Fietje, Research Officer at WHO/Europe, added, “We are delighted to see that the work being done in the WHO European Region can be of use and inspiration elsewhere. It has become abundantly clear that health insights on matters such as culture are a critical component to finding solutions that are contextually integrated and thereby fit for purpose.”
Ted Fischer, Cornelius Vanderbilt Professor of Anthropology and Director of the Center of Latin American Studies, will lead the work. Fischer has served as an external advisor for WHO/Europe on topics of culture and health over the last 4 years.
“The medical field has been moving toward a model of considering the whole person, not just the disease, for a while now, and this project presents a great opportunity to rethink how we do medicine in ways we might not have considered before,” Fischer said. “And that’s really exciting.”
WHO project on cultural contexts of health and well-adopted in U.S.
Robert Wood Johnson Foundation
Sunday, July 19, 2020
Creating Value Worlds with Third Wave Coffee
Interview with Society for the Advancement of Socio-Economics: https://sase.org/uncategorized/quality-and-inequality-creating-value-worlds-with-third-wave-coffee/
Wednesday, July 8, 2020
Cultures of Health and Sickness in the COVID Era - Le Monde Diplomatique
Cultures of health and sickness
A. David Napier and Edward F Fischer
- https://mondediplo.com/2020/07/04uganda
A group of researchers, led by David Mafigiri at Makerere University in Uganda, began collecting data this January for a long-planned health vulnerability assessment to identify what makes people and communities more vulnerable or resilient to infectious diseases. This study was in place well before the Covid-19 pandemic as part of Sonar-Global, a European Commission-funded research programme, and the team could amend questions based on current developments.
The data is now being analysed. But it is clear that, since lockdowns are still in place globally for fieldworkers and there is a hold on almost all face-to-face public health research, Uganda may have the only systematic real-time data on how people in at-risk communities conceptualise and respond to the virus.
The information the assessments collected is notable. The interviews lasted between one and three hours, much longer than a normal health survey. Instead of taking blood samples and asking multiple choice questions, researchers met participants in their homes and had structured but wide-ranging conversations about access to services, about availability of medical care and other health-related information, and about local conventions, practices and norms — ‘culture’.
Why culture? And why invest time and effort on things apparently unconnected with health and infectious disease? Because infectious viruses are about social networks and cultural norms, as much as about microbes. As science tells us, viruses are inert, unable to attack us. We transmit viral data though our social networks and cultural pathways. We give viral information to each other by how we live and what we do. Otherwise viruses just sit inert, sometimes for thousands of years. So understanding cultural contexts is just as important as sequencing genomes in tackling viral outbreaks.
Culture is nonetheless downgraded. Most of the time, when medical researchers try to work culture into their models, they fall back on tired stereotypes about local beliefs as obstacles to biomedical care, a supposed opposition of culture and science. In this paradigm, social scientists are lined up to help ‘real’ scientists determine why culture keeps others from doing what’s medically recommended.
A broader understanding of culture recognises its varied potential. Though clinicians may see culture as an obstacle to health, it is also a source of enduring trust. Moreover, it is not just something ‘they’ have: healthcare providers, scientists and policymakers all have their own cultures of practice, which inform their unique perspectives and encourage them to work together.
Cultures of practice However, the underlying and often taken-for-granted assumptions of culture about what is feasible can also limit innovative thinking. That’s why we use the word culture pejoratively to describe the intransigence of institutional cultures, political, academic or professional. In this sense, accounting for the cultural contexts of health and wellbeing is a primary health determinant — why ‘the systematic neglect of culture in health and healthcare is the single biggest barrier to the advancement of the highest standard of health worldwide’. That’s because culture is, in fact, the key to addressing health equity, especially when providers and target populations operate under different shared understandings about what matters most biologically and socially.
Thus, a cultural context of health approach is critical in responding to Covid-19. Because governments not previously concerned about health equity feel they must blame others for the impact of their own negligence. Because thinking of Covid-19 as only a medical challenge fuels xenophobic fears about outsiders. Because humanitarian action groups talk about working with communities even as inequalities within communities are exacerbated by the crisis. And because, given the socially sanctioned, chronic neglect of citizens already on the margins, Covid-19 pushes those on the edge into overt calamity coping. The taken-for-granted assumptions of cultures of practice give us a sense of belonging and trust, but sometimes blunt creative thinking and social innovation. For our assumptions help little in times of uncertainty. We know this because, when a disaster happens, so many show up late and with outdated equipment.
What can a cultural understanding of Covid-19 vulnerability tell us? We don’t need more research to recognise that the elderly, the homeless and unemployed single parents are especially at risk. They’re already vulnerable socially and economically, and, to our shame, become even more so when their fragile survival strategies are even more challenged.
But inequalities are always exaggerated in a crisis, and then many initially less vulnerable people are also pushed across capability and opportunity thresholds and into conditions of real peril.
That is why Uganda can now tell us more than we might expect. To understand what is happening in real time with real people, we need, as did David Mafigiri, to assess vulnerability before a disaster; like his own research team in Uganda, we need an extant interest in the disadvantaged. Ongoing empathy is critical. Without that, you have no access to what you should have known and now can’t. Your belated concern rings hollow in the face of that failure, which makes you liable to blame others. Indeed, organised humanitarian action all but stops in Covid-19, as we have little way of knowing what’s really happening on the ground among those most vulnerable, who live alone and without access to online services.
In response to such new instability, the World Health Organisation (WHO) rightly wants a ‘Just Recovery from Covid-19’. That, of course, is critical. But what we need equally is a just preparedness before an epidemic. We have to do the hard work of creating cultures of trust and solidarity in advance, and resist salvation narratives in which epic actions create save-the-world medical heroes and destructive villainous viruses.
In welfare states, where trust in government has remained relatively stable, there are few heroic stories, because stability and a commitment to the common weal lessened the need for bombast well before Covid-19 incited it. Initiatives such as Cities Changing Diabetes (a Danish community engagement strategy sponsored by Novo Nordisk) demonstrate how prior work around understanding health vulnerabilities translates, despite its focus on a non-communicable disease, into actionable understanding in the crisis. That is because the programme has been assessing global health vulnerabilities since 2015, years before Covid-19.
New vulnerabilities Vulnerability emerges variably, at different times and places. This means that, while already vulnerable populations become even more so under stress, new vulnerabilities emerge that often outstrip old ones. Service industry employees without health benefits and dependent on daily income become more vulnerable, especially where they now have to go back to work, than those elderly who can stay at home and wait it out. High-income physicians without adequate protective gear are as vulnerable as those with chronic pre-existing conditions. Places we previously thought of as havens are anything but: in Europe and the US, the most vulnerable are in ‘care’ institutions: nursing homes, shared housing, prisons.
We failed these vulnerable groups because their illness experiences are socially driven, and that is too often separated from health. We look instead for specific risk factors in isolation without seeing how compounding, already-existing, stressors push populations into extreme vulnerability during a crisis — especially those with few choices and nowhere to go. In the UK, ethnic minorities are dying at higher rates from the virus than the rest of the population; and in the US, African Americans have far higher mortality rates than white and Asian American populations. Yet, as crises widen existing rifts in societies, they also open up opportunities for communities to come together in ways unthinkable in normal times; in Rio de Janeiro, for instance, gangs in several favelas imposed shelter-in-place orders to reduce transmissions.
Communities must often adapt on their own, because political systems are vulnerable to pandemics too: the global crisis is making clearer what is important at national and local levels, and what is less so. It shows us what we collectively value, and makes us reconsider often-tacit assumptions. Indeed, our judgments of what is essential have also changed across the globe, providing a singular opportunity for institutions and governments to rebalance private gain and public good.
This adjustment can go either way. On the one hand, speaking of the virus as a foreign enemy incites xenophobia, with the social category of ‘insider’ — the ‘we’ in ‘we are all in this together’ — getting smaller and smaller. On the other, the pandemic has catalysed new alliances, as with Black Lives Matter and anti-police protests. Mistrust in the institutions of government may be the only thing uniting the far right and far left in countries like the US and Brazil.
That is why ‘just preparedness’ matters, and also why Uganda might lead the way in understanding the human impact of Covid-19. Because this pandemic is not just about an infectious threat, but about the urgency of caring beforehand, and about the steep decline in social trust that emerges quickly in unequal settings where global neoliberal economics have undermined public wellbeing.
Fortunately, that decline has created opportunities in surprising places. Gangs in favelas may seem a stretch when policymakers think about health systems change, but some far-sighted private companies have been quicker than many governments to recognise and respond to shifting public sentiment: sending their employees to work from home, speaking out against racism and calling for more government guidance. However, not all businesses are equal: companies less vulnerable to shareholder pressure to maximise short-term profits are better able to consider their potential long-term future roles, and not just in the next quarter — recognising that an economy cannot survive unless nation states and their citizens have stability, enough income, and access to robust and well-funded care.
Mistrust in business There have been calls by world leaders, including Ursula von der Leyen, head of the European Commission, for a new Marshall Plan to improve abysmal levels of trust in business recorded by Richard Edelman’s Trust Barometer. But that mistrust can only be reversed by sustained long-term commitments that are faithful to a range of stakeholders — including employees, clients and the social and natural environments we all depend upon for survival.
Divisive political leaders, like Donald Trump or Brazil’s Jair Bolsonaro, may blame the left, or the Chinese, or the CIA for Covid-19, based on alternative, often paranoid political narratives that divide local communities. That is because for opportunists, big or small, the crisis remains an intractable intrusion into populist narrative worlds built on political delusion. But the virus’s deadly materiality resists rhetorical defences and counter-factual denials, even if some seem intent on taking the ship down, or watching it sink while drowning in denial. The states lacking welfare can only blame others.
Social trust and faith in institutions are therefore crucial for the collective actions required to halt viral transmission. We have to coordinate our social behaviours in uncomfortable, inconvenient, and even personally painful ways. They are vital to collective wellbeing and require sacrifice; a sense of commonality and social solidarity must be based around shared values — culture. A crisis in governance, correlates with, and can be directly mapped onto, a crisis in trust, because where we find trust is key.
As the US pulls support from the WHO, there is a serious question: where do we go for an independent and trustworthy adjudication on health risk? The world’s biggest healthcare charity, the Gates Foundation, has always espoused magic bullet answers to health problems and is uninterested in the complex social drivers of our wellbeing. The Centers for Disease Control is a US federal agency that works well in good times but in bad times is vulnerable to partisan political nonsense. Without socially trustworthy institutions, how are we to respond to growing uncertainty?
Sustained uncertainty And how, finally, can we learn to deal with sustained uncertainty and the psychological vulnerability it causes? If many governments cannot lead equitably, and viruses are just information we share, there must be other drivers of Covid-19 we can act on. Other factors remain under-represented: the more people there are on the planet, the more often viruses like Covid-19, which are more contagious but less lethal than Ebola, will connect us. And that is a big problem, not only because science, in the absence of a vaccine, still medicalises a pandemic almost entirely driven by our social responses, but because there are more of us to circulate and adapt to that viral information.
This really matters with Covid-19, since, if lasting immunity doesn’t happen soon, we need to rethink the social contract in ways that run counter to those who advocate for biodeterminism or xenophobic scapegoating or maximising self-interest. Otherwise, when the pandemic abates even temporarily, we risk going back to ‘normal’, forgetting what we might have learned until the next infectious disease outbreak, when we will again be completely surprised by what we should have expected. We need to consider the needy before that happens — to put heart and soul into thinking about both how we live together with uncomfortable uncertainty, and how we address together the social and cultural drivers of health vulnerability.
A David Napier is professor of medical anthropology at University College London, innovations lead for Sonar-Global, global academic lead for Cities Changing Diabetes and international chair of the Robert Wood Johnson Foundation committee on the Cultural Contexts of Health and Wellbeing initiative. Edward F Fischer is professor of anthropology and health policy at Vanderbilt University in Nashville, Tennessee, where he also directs the Center for Latin American Studies and the Cultural Contexts of Health and Wellbeing initiative.
Copyright ©2020 Le Monde diplomatique — distributed by Agence Global
—————-
Released: 07 July 2020
Word Count: 2,139
—————-

Friday, May 1, 2020
Monday, November 12, 2018
‘Now is the Time of Monsters’: The Painful Birth of a New World Order
President Trump calls the WTO a “disaster” and NATO “obsolete,” and seasoned diplomats and foreign policy experts react with reasoned disdain and moral contempt. His tweets and remarks are said to be reckless, needlessly destructive, and further proof—as if any were needed—of the president’s lack of both capability and character. Whatever you make of his latest episodes, Donald Trump’s behavior is certainly disruptive—and, as progressives have argued, our outdated economic and political systems need a little shaking up. While Trump does not offer any positive alternatives with his populist takedowns, his disruptions create an opening for a new sort of world order to emerge.
The rules-based international order relies on political structures designed for a different era and built up over two twentieth-century waves of growth and prosperity in the West, the Trente Glorieuses following WWII and the 30 years of neoliberal globalization following the fall of the Berlin Wall. But these structures are ill-suited to the technological and economic realities of the post-millennial world.
“The old world is dying away, and the new world struggles to come forth,” observes Slavoj Žižek, paraphrasing Gramsci. “Now is the time of monsters.” While we may disagree with his solutions, and we may not like his style, President Trump is not wrong to question the UN and NATO, the IMF and World Bank, WTO and NAFTA, and other structures of twentieth-century globalization. NATO is built on the idea of a wall running down the middle of Germany that has not been there for almost 30 years. The UN rests on a notion of sovereign nation-states at odds with the explosive growth of diaspora populations and the power of non-state actors. Trump dislikes these Cold War-era institutions for disagreeably nativist reasons, but his opposition converges tightly with progressive skepticism.
The reality is that the post-millennial world has outpaced our understanding of it. A new global order is emerging, with more flexible dynamics and multiple centers of state and non-state power. Our leaders largely lack the conceptual and political tools to deal with it, but anthropology offers some key insights.
While it is unclear exactly what the new rules will be, China will play a preeminent role. They have replaced the U.S. as the world’s strongest pro-trade voice for globalization, taken the lead in international climate change efforts, and started an ambitious (strings-attached) international development program, One Road, One Belt. The country’s Asian Infrastructure Development bank is now capitalized at half the amount of the World Bank and gaining rapidly, while the Made in China 2025 is on track to achieve global dominance in key manufacturing sectors.
This is not just a story of China’s rise, however, but also of the emergence of a more fluid and diffuse international power structure generally. Recent polls show that Germany has replaced the U.S. as the world’s most respected country. Meanwhile Russia flexes its muscles by sending comically veiled signals, brazenly poisoning defectors and riling up the social media fringes.
It’s also a story of the rise of functionally sovereign non-state actors. Many, like the narco-traffickers of Guatemala and Honduras, not to mention Al Qaeda and ISIS, are better armed and more powerful than the governments. Or their power may be financial: East European cybergangs regularly hold not only hapless individuals but whole police departments and city governments hostage with ransomware, extracting payment in Bitcoin or other virtual currencies. Which leads to the realization that while the dollar is likely to remain the world’s reserve currency for some time, the curtain has been pulled back and governments have lost their mystical monopoly on the creation and control of money. Meanwhile, independent entities like the Gates Foundation, the Koch brothers and large transnational corporations like Apple, an American company whose stateless billions are stashed away in Irish banks, are supplanting, influencing, and circumventing governments in ways (good and bad) that we don’t have the tools to address.
We need a political understanding of the world that accounts for not just the emergence of these non-state actors but burgeoning diaspora populations as well. International migration to high-income countries increased by almost 90 percent since the fall of the Berlin Wall. Never have we seen such massive movements of people around the world, but our governance structures are ill-equipped to represent Syrian refugees in Europe, Filipino workers in Qatar, or Kurds anywhere. We need frameworks that can account for cultural communities that may be only loosely connected to a geographic place.
Bucking conventional economic wisdom and Republican orthodoxy, Trump sees trade as a zero-sum game in which there are losers as well as winners. Social-justice opponents of free trade largely concur, pointing out that such deals hurt smallholders and local producers (of corn in Mexico, for example) as well as dismantling the livelihoods of U.S. factory workers. While they have different victims in mind, Subcomandante Marcos and Donald Trump both see free trade pacts as mechanisms for the economic exploitation of those already in precarious circumstances.
Trump’s approach to trade deals seeks to protect certain sorts of jobs, the jobs of twentieth-century white working-class prosperity. But this idea is as retrograde as the global institutions themselves. A more forward-looking solution would be to support workers (rather than job categories) through inevitable transitions. Even that may not be enough to address the possibility of a crisis within capitalism itself, or the attendant social and political disorder, if the shiny diversions of social media prove insufficient distractions from the material realities.
In the current age of consumer capitalism, we are so inundated with attempts to shape our opinion that ironic distance can simulate critical analysis and Trevor Noah becomes the voice of informed reason. With all that is solid melting into air, Trump begins to sound like an alt right Baudrillard in his critiques of the social construction of “truth,” fueling disillusionment with a political-economic system that wide swaths of the U.S. electorate see as stacked against them.
In this context, Trump’s openness about “the system” being a system (that can be gamed) and his transactional view of relationships makes his insincerity come off as authentic. It also reveals an intuitive grasp of critical theory: understanding that the institutions of capitalism and democracy are human creations can empower us to make them suit our ends rather than conform ourselves to theirs. The progressive left needs to recapture this insight to offer bold, positive alternatives to outdated systems. It is time to put down the rocks and pick up a hammer.
Thursday, November 8, 2018

Tuesday, November 6, 2018

Thursday, November 1, 2018

Friday, March 30, 2018
Thursday, December 28, 2017
Economy, Happiness, and the Good Life: An Interview with Edward F. Fischer
 |
| GB. England. New Brighton. From ‘The Last Resort,’ 1983-85, Martin Parr. |
KR: What do you understand by the notion ‘the good life’?
Edward F Fischer: I see you are starting off with the trick questions. A large part of the attraction of the phrase is precisely its semantic slipperiness and strategic ambiguity. We may all agree . . . continue at http://kingsreview.co.uk/articles/economy-happiness-good-life-interview-edward-f-fischer/
Tuesday, October 18, 2016
Eating Identity: Nourishment and the Cultural Contexts of Food

We eat for nourishment, but food is about much more than nutrition. What we eat is meaningful, and food is an especially intimate area of daily life, tightly linked to our conceptions of self. Think about your own food preferences: a nostalgic meal from your childhood, a treat you indulge yourself with on special occasions, a religious sanction against certain foods. In these ways, food is not only at the heart of our material subsistence, it is at the core of our identity as well, deeply associated with family, hearth, home, and community. We are what we eat, conceptually as well as biologically.
Understanding this becomes especially important when we look at nutrition from a public health perspective. In a situation that would have been unimaginable for most of human history, over-nutrition has become one of the biggest problems for health and chronic diseases in many parts of Europe and the U.S., eclipsing smoking as public health enemy #1. The chronic and non-communicable diseases that are the big burden these days (heart disease, cancer, diabetes, stroke) are often connected to diet.
The WHO’s Health 2020 report advocates people-centered approaches to public health, looking at both the whole person and the whole society. This is especially relevant for nutrition because it is so connected to different aspects of life, from our cultural and idiosyncratic preferences to state subsidies and agricultural policy.
Poor nutrition is not just an over-abundance of macro-nutrients or a deficiency of micro-nutrients: it is based on cultural traditions and personal histories; the natural environment and geographies of inclusion and exclusion; about large food corporations and grocery store marketing as well public policy and regulations. This is to say that both structural conditions and cultural practices affect nutritional choices.
Thinking of food and identity, what comes to mind first might be kosher or halal cuisines, or perhaps vegetarian or vegan preferences. These are certainly important aspects of religious and social identity, but the link works at a much more mundane levels as well. Our quotidian food choices reflect our preferences and values, and identity: eating organic (or not), eating fast food (or not), liking broccoli (or not), and so on.
Since food is so integral to identity, it is tricky to tinker with. And food choices not only reflect identity, but identities can become literally embodied through eating. For example, many Maya people in Guatemala claim not feel full unless they eat corn tortillas (often a dozen or more with every meal); I have heard Germans claim the same feeling and physical craving for black bread.
Eating is also usually a group activity, and as such a primary site for socialization, family binding, and group identity reinforcement. Yet nutritional recommendations often focus just on the individual. And since individual choices affect others, change cannot happen with just the individual, it would involve the whole family.
And just as eating is a group activity, also provisioning is often an expression of love and caring. Anthropologist Daniel Miller has show how food treats are especially important in this regard: choosing for significant others what they might want. Miller shows that grocery shopping, far from the hedonistic indulgence that the term “consumerism” invokes, is more about provisioning for one’s family, expressing one’s concerns for loved ones.
Packaged and processed foods are a big contributor to poor nutrition, and so are deservedly the target of ire among nutritionists and public health advocates. A number of efforts to impose a “soda tax” have been tried around the world; in Mexico it has had a dramatic and measurably impact in just a few years. All the same, we should also recognize that such foods are one of the few affordable luxuries for poor families, a way to demonstrate their love for their children when they cannot give them much else. It is well and good to try to curb snack food consumption, but keep in mind that it may be more than a snack that has to be changed.
Finally, when we talk about the health impacts of nutrition, we often reduce eating down to certain numbers. My colleague Emily Yates-Doerr, in her book the Weight of Obesity, calls this the metrification of diets: the number of calories and grams of fat, the percentages of daily allowances for vitamins and minerals. This metrification reduces the richness of eating and the sociality around it to these metrics of macro- and micro-nutrients. Many of us have become accustomed to this way of thinking about food, reading labels on the fly in the supermarket. Food and eating is about love and identity as much as calories, but how do we translate “love” into grams or ounces?
Just because something is supposed to be “good for you” is often not enough to change behavior. Diet and food choices need to be looked at holistically, as part of broader lifeways and family and social networks. Labeling regimes can inform consumer decisions and move the market, and soda taxes and other nudges can make a difference, but ultimately public health programs working on nutrition need to engage people through their customs and beliefs rather than work at odds with them.
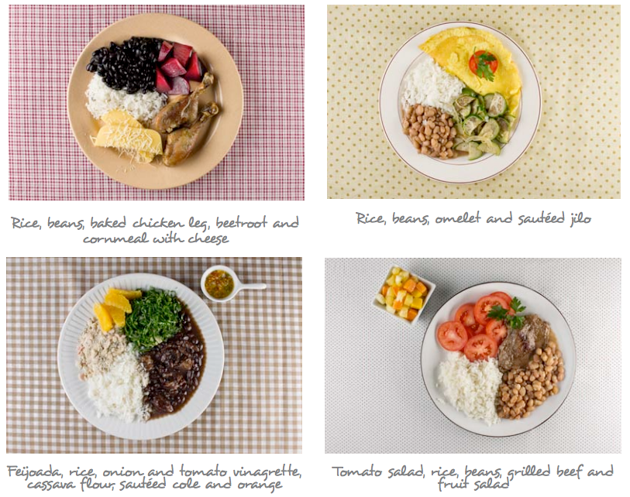
In an innovative approach, Brazil has adopted what they call “food-based” dietary guidelines that seek to build on cultural norms and preferences rather than fight them. Rather than giving percentages recommended for different foodstuffs (as with the traditional food pyramid), Brazil adopted 10 broad principles and illustrate them in public service ads in terms of a plate prepared for a typical meal.
- Make natural or minimally processed foods the basis of your diet
- Use oils, fats, salt, and sugar in small amounts
- Limit consumption of processed foods
- Avoid consumption of ultra-processed foods
- Eat regularly, deliberately, and with others
- Shop in places that offer a variety of natural or minimally processed foods
- Develop, exercise and share cooking skills
- Plan your time to make food and eating important in your life
- Out of home, prefer places that serve freshly made meals
- Be wary of food advertising and marketing
Sunday, August 21, 2016
Third Wave Coffee and the Formation of Taste (and Value)
-->
 In 2015 the SCAA unveiled a new flavor chart for specialty
coffee. Working with researchers at UC Davis and Kansas State, the Coffee
Taster’s Flavor Wheel offers a lexicon of coffee terms coming from “the
frontiers of sensory science methods and analyses.” They described the process
using technical language (“an Agglomerative Hierarchical Cluster (AHC) analysis
was performed on the results from the sorting exercise to group the flavor
attributes into different categories (or clusters) represented visually by a
dendrogram”) (Sage 2016).
In 2015 the SCAA unveiled a new flavor chart for specialty
coffee. Working with researchers at UC Davis and Kansas State, the Coffee
Taster’s Flavor Wheel offers a lexicon of coffee terms coming from “the
frontiers of sensory science methods and analyses.” They described the process
using technical language (“an Agglomerative Hierarchical Cluster (AHC) analysis
was performed on the results from the sorting exercise to group the flavor
attributes into different categories (or clusters) represented visually by a
dendrogram”) (Sage 2016).
“Orange blossom, white tea, syrupy”
“Grapefruit, spicy pepper, olive oil”
“Chocolate, red berries, roasted barley”
The language used to talk about new high-end coffee comes
straight out of the wine world, with exotic and evocative descriptors and even
a 0-100 grading scale (à la Robert Parker). Scores above 80 mark “specialty”
coffee (such as would be served at Starbucks) and scores in the high 80s and
breaking 90 place beans in the rarefied world of Third Wave coffees that retail
for $5, $6, $7 a cup and more than $25 a pound for roasted beans (although
usually sold in 12oz, or increasingly 6oz, packages to both stress the limited
supply and make the price tag slight less eye-popping).
Virtually all high-end coffees are of the species Arabica;
among Arabicas there are a range of different varieties. A growing number of
exclusive lots of green coffee have sold for more than $100 a pound, a ceiling
first broken in 2007 by the storied Geisha varietal from Hacienda La Esmeralda
in Panama. In 2012, a Mocca (a heirloom varietal originally from Yemen) grown
by the Finca El Injerto in Guatemala sold for $500.50 a pound, still a record.
(Meanwhile, the commodity price for quality washed Arabica, known as the New
York C price, has fluctuated between $1.13 and $1.46 over the first 8 months of
2016)
Are these coffees worth that much? People often ask me this
when I talk about Third Wave coffee. If you haven’t tried one yet, it is a
different experience than either the office kitchen’s K-cup or even a solid cup
of coffee from most neighborhood coffee shops. A whole range of subtle flavors
come out in the clean, smooth, balanced cup profile; sugar and milk are,
naturally, verboten.
Yes, but are they worth the high price? It depends on how we
value them. In high-end markets that move toward singularity (limited edition
prints, that particular Bordeaux vintage, the 2012 El Injerto Mocha), normal
market forces of supply and demand don’t apply. Which leads us to consider what
constitutes value for such non-commodities and how do we put a price on that.
Objective quality (by established tasting standards and
conventions) and market scarcity play an important role, but we cannot discount
the symbolic values at play: the relative positioning of conspicuous
consumption; the imagined, personal relationship with a producer; and
underwriting it all, the cultural and market shift among the global affluent
toward artisanal and singular products. The language used to talk about Third
Wave coffee borrows heavily from fine wine, ideas of terroir, and the artisanal
food movement. And this provenance, these narratives, are key to its value.
Three Waves
The first wave of coffee consumption lasted from the late
nineteenth century up through the 1960s, marked by the spread of commodity
coffee and the rise of Folgers, Maxwell House, and all the other familiar
grocery store brands.
The second wave started in the 1960s in the U.S. with Peet’s
in San Francisco and Zabar’s in New York, and culminating in the spread of
Starbucks to every nook and cranny of the country, and increasingly the world.
Anthropologist William Roseberry describes this as a shift from coffee as being
the beverage of capitalism (coffee and sugar serving as great proletarian
hunger killers, as Sidney Mintz has pointed out) to being a beverage of
postmodernity (an outlet for performing identity and difference).
The Third Wave coffees take this to the next, artisanal
infused, level. Coming out of coffee shops in Portland, Brooklyn, San
Francisco, Nashville, Washington, Philadelphia, and other cities, Third Wave
has both hipster and foodie associations; it is sold by online retailers such
as Stumptown, Intelligentsia, and Blue Bottle.
Creating Taste and Value
The Specialty Coffee Association of America (SCAA, the trade
group for specialty and Third Wave coffee) goes to great lengths to bolster the
scientific credibility of its classifications and tasting protocols. The more
objective they seem, they more they can impart the power of authenticity
(discovering something rather than constructing it).
The SCAA-associated Coffee Quality Institute certifies
coffee cuppers with its Q Grader certification, with applicants having to pass
five “triangulation cuppings” to differentiate a total of 90 distinct coffees.
A Roast magazine article on the
allure of triangulated cupping, observes that even a novice will quickly learn
to distinguish coffees from different world regions, then so after by country.
For example, “a Latin American coffee is going to taste different than an
African coffee,” and tasting them side by side reveals the differences. “Put an
Ethiopia Harrar into two cups and Sumatra Mandheling in one cup, and you will
know the difference,” the article claims. Or, at least, you will learn the
differences in going through a cupping protocol. One Portland roaster loved
“the earthiness of the Sumatra” and another noted that Central American coffees
are known for an exceptionally clean acidity (Allen 2010: 58).
 In 2015 the SCAA unveiled a new flavor chart for specialty
coffee. Working with researchers at UC Davis and Kansas State, the Coffee
Taster’s Flavor Wheel offers a lexicon of coffee terms coming from “the
frontiers of sensory science methods and analyses.” They described the process
using technical language (“an Agglomerative Hierarchical Cluster (AHC) analysis
was performed on the results from the sorting exercise to group the flavor
attributes into different categories (or clusters) represented visually by a
dendrogram”) (Sage 2016).
In 2015 the SCAA unveiled a new flavor chart for specialty
coffee. Working with researchers at UC Davis and Kansas State, the Coffee
Taster’s Flavor Wheel offers a lexicon of coffee terms coming from “the
frontiers of sensory science methods and analyses.” They described the process
using technical language (“an Agglomerative Hierarchical Cluster (AHC) analysis
was performed on the results from the sorting exercise to group the flavor
attributes into different categories (or clusters) represented visually by a
dendrogram”) (Sage 2016).
The flavor wheel ranges from Chamomile, Rose and Jasmine to
Vegetative and Herblike to Petroleum, Skunk, and Pipe Tobacco.
In order to calibrate such flavors, the accompaning guide
gives references to ground a 0-15 scale of intensity. For example, one entry
reads:
BLACKBERRY: The sweet, dark, fruity,
floral, slightly sour, somewhat woody aromatic associated with blackberries
REFERENCE: Smucker’s
Blackberry Jam
INTENSITY: 5.5
PREPARATION: Serve
jam in a 1-ounce cup. Cover with a plastic lid.
Recently, among trendsetters there has been a shift in
preference away from the more traditional deep, creamy chocolate flavors (and
maple syrup, caramel, red wine) toward more floral and citrus notes.
The Cup of Excellence program has taken cupping
standardization to the next level, as my colleague Bradley Wilson has observed.
In Cup of Excellence competitions, each coffee will be blindly evaluated 5
times by different cuppers. Only coffees
that get consistently high scores advance in the competition, and out of
hundreds of entrants each country will have 25-35 ranking winning coffees that
are sold at a live internet auction.
Guatemala is ground zero for Third Wave coffee. This is due
in part to its unique geographic and climatic endowments. High altitude coffees
tend to command higher premiums, and Guatemala’s volcanic slopes and varied
microclimates create a range of subtle flavors. But it was also visionaries
such as Bill Hempstead, who as president and a director of the Guatemalan Coffee
Association (Anacafé), promoted the branding of regional cup profiles which has
led to the flourishing of single estate and micro-lot coffees.
Saturday, August 20, 2016
Broccoli, Anthropology, and the Humanities
Broccoli, Anthropology, and the Humanities: Caitlin Patton discusses how the work of Ted Fischer, an anthropologist focused on food culture, specifically the cultivation of broccoli in Guatemala, inspired her choice to study at Vanderbilt University.
Monday, August 1, 2016
Imagining the Future & Economic Fictions
“The tradition of all dead generations weighs like a nightmare
on the brains of the living,” Marx remarked in The Eighteenth Brumaire, and although we may all make our own
futures, we do not make them just as we please. For such reasons, we social
scientists tend to look to the past to explain the present, to show the particular historical trajectory that led things
to be the way the are. All the same, privileging the past can allow us to forget that
people in the present are not trying to (just) recreate yesterday, but have an
eye toward tomorrow and next year and the lives of their children and
grandchildren.
Unlike Marx’s vivid prose, today the dismal science (qua
science) often forgets about the human passions behind their numbers. In the
sterile statistical world of GDP and interest rates, it is easy to loose sight
of the hopes and dreams, the aspirations and fears—what Keynes termed our
“animal spirits”—and the individual lives behind all economic transactions.
In a remarkable new volume, Jens Beckert (Imagined Futures: Fictional Expectations and
Capitalist Dynamics) moves us toward conceptually linking the passions and
animal spirits of lived experience with a macro-understanding of the workings
of capitalism. He does this by focusing on the future, and the fictive
qualities of imagining the future that underwrite capitalist dynamics.
In this meticulously researched and engagingly written
volume, Beckert uncovers the role of imagined futures as a fundamental driver
of capitalism. It is the sort of observation that makes complete sense when you
hear it, but that has gone largely unremarked upon until now. He shows that the
future orientation of capitalism is based on competition and credit,
fundamental elements at the very core of the financial system. (I would add,
also the construction of desires, especially in late capitalist formations.)
The financial system is built on credit, and demands continual expansion and
continual returns. We are all in bad shape if growth stops, as our retirement
and much of our insurance depends on markets continuing to expand—not to
mention our subjective hopes and dreams.
Beckert makes the provocative point that a lot of what we
consider to be risk (and thus manageable, knowable, predictable) is actually
uncertainty. We make up stories about the future, and convince ourselves and
others that these are more or less likely (in a statistically predictable
manner). For example, investment in innovation requires collectively deciding
to believe in a fictional future. And, as with innovation, imaginaries can
create structures that make real the fictional expectations (186).
In the realm of consumption, Beckert identifies two key
types of symbolic value: (1) positional and (2) imaginative. Positional values
(first observed by Veblen) derive from the scarcity of a good and how many
others have it; rather than absolute material utility, the positional value of
a good is only given by its relation to other goods. With imaginative value, “a
good functions as a link between subject and her desired but intangible ideals”
(195). Imaginative value gets at what it means to the person herself, more than
just positional/status importance. With imaginative value, a good embodies
something transcendent.
Berkert’s new book is exhilarating, opening up new
possibilities for thinking about (and acting on) the market. It gives us a way
to insert the social and the cultural back into the fundamental mechanics of
capitalism, from wince it has long been banished.
Jens Beckert’s Imagined
Futures: Fictional Expectations and Capitalist Dynamics. 2016, Harvard U Press.
Friday, November 13, 2015
Q&A: Ted Fischer of Vanderbilt | Nashville Post
Read the Nashville Post's Q&A: Ted Fischer of Vanderbilt on Social Entrepreneurship and Mani+
Ted Fischer is professor of anthropology and director of the Center for Latin American Studies at Vanderbilt University. Over a five-year period, he teamed with Steve Moore (head of Middle Tennessee-based Shalom Foundation) and multiple VU students on a malnutrition-oriented and social enterprise effort called NutriPlus, which produces the supplement, Mani+.
The supplement (a fortified nut paste that provides calories, protein, fat, vitamins and minerals essential to brain development in babies and toddlers) is used to specifically address the nutritional deficiencies seen in Central American children. It is the first ready-to-use supplementary Food (RUSF) to be both locally produced and locally sourced in Guatemala City, Guatemala, creating local jobs and supporting local farmers.
The new facility (read more here) opened on Sept. 23 and will eventually mass produce Mani+. Eventually, Fischer and Moore hope to produce 25 tons of Mani+ a month, reaching about 25,000 children.
Post Managing Editor William Williams recently chatted with Fischer regarding the effort.http://nashvillepost.com/blogs/postbusiness/2015/10/19/qa_ted_fischer_of_vanderbilt
Ted Fischer is professor of anthropology and director of the Center for Latin American Studies at Vanderbilt University. Over a five-year period, he teamed with Steve Moore (head of Middle Tennessee-based Shalom Foundation) and multiple VU students on a malnutrition-oriented and social enterprise effort called NutriPlus, which produces the supplement, Mani+.
The supplement (a fortified nut paste that provides calories, protein, fat, vitamins and minerals essential to brain development in babies and toddlers) is used to specifically address the nutritional deficiencies seen in Central American children. It is the first ready-to-use supplementary Food (RUSF) to be both locally produced and locally sourced in Guatemala City, Guatemala, creating local jobs and supporting local farmers.
The new facility (read more here) opened on Sept. 23 and will eventually mass produce Mani+. Eventually, Fischer and Moore hope to produce 25 tons of Mani+ a month, reaching about 25,000 children.
Post Managing Editor William Williams recently chatted with Fischer regarding the effort.http://nashvillepost.com/blogs/postbusiness/2015/10/19/qa_ted_fischer_of_vanderbilt
Thursday, October 1, 2015
Friday, September 4, 2015
Health, Culture, and Wellbeing: Beyond Seeing Culture as Obstacle
The World Health Organization (WHO) defines health as “a complete state of physical, mental and social well-being, and not merely the absence of disease or infirmity.” And yet, for much of its history, it has (understandably) focused on eradicating disease and infirmity. There is a move afoot with the WHO to focus more on wellbeing as broadly conceived in its charter. Nils Fietje and colleagues at WHO-Europe have been looking lately at “Cultural Determinants of Health,” a project I have advised.
While there is a growing understanding that “culture” plays a crucial role in health and development, the concept as it is invoked generally relies on very traditional definitions. Common definitions of culture in public health understand it to be “shared values, beliefs, and practices.” Note that here “culture” is used as a noun, denoting bounded groups defined by lists of traits.
But we should see cultural forms as opportunities, not as obstacles, to health
A human-centered approach to health and wellbeing, should adopt contemporary understandings of culture as dynamic, future oriented, and driven by agency. We in anthropology now see culture as much more of a fluid process, a process rather than a thing. Cultural actors are always improvising, actively creating meaning out of the resources at hand.
We have also traditionally put too much emphasis on the historical determinants of culture and adherence to tradition. My view is that we should think of cultural orientations not just as not endowments but as future-oriented desires. Arjun Appadurai defines culture as “a dialogue between aspiration and sedimented traditions.”
In this view, culture opens the door for new opportunities for engaging communities and understandings of well-being.
The full report in English and Russian is at: http://www.euro.who.int/en/data-and-evidence/cultural-contexts-of-health/beyond-bias-exploring-the-cultural-contexts-of-health-and-well-being-measurement
While there is a growing understanding that “culture” plays a crucial role in health and development, the concept as it is invoked generally relies on very traditional definitions. Common definitions of culture in public health understand it to be “shared values, beliefs, and practices.” Note that here “culture” is used as a noun, denoting bounded groups defined by lists of traits.
What is missing from such definitions is the human element: real human beings constructing their lives in active and dynamic ways. The traditional static definition (the most common one deployed in public health contexts today) usually portrays culture as an obstacle to health.
But we should see cultural forms as opportunities, not as obstacles, to health
A human-centered approach to health and wellbeing, should adopt contemporary understandings of culture as dynamic, future oriented, and driven by agency. We in anthropology now see culture as much more of a fluid process, a process rather than a thing. Cultural actors are always improvising, actively creating meaning out of the resources at hand.
We have also traditionally put too much emphasis on the historical determinants of culture and adherence to tradition. My view is that we should think of cultural orientations not just as not endowments but as future-oriented desires. Arjun Appadurai defines culture as “a dialogue between aspiration and sedimented traditions.”
In this view, culture opens the door for new opportunities for engaging communities and understandings of well-being.
The full report in English and Russian is at: http://www.euro.who.int/en/data-and-evidence/cultural-contexts-of-health/beyond-bias-exploring-the-cultural-contexts-of-health-and-well-being-measurement
Wednesday, July 1, 2015
Voting for Our Better Selves; and Rules to Flourish By
Mike Pesca, in one of his artful spiels on The Gist podcast, punctures the conventional wisdom that we Americans want folksy presidential candidates, that we yearn for a leader just like us, someone we can relate to, imagine having a beer with. While we do like candidates to be down-to-earth (perhaps echoes of our anti-monarchical national origins), Pesca convincingly argues that what we really want is not a leader like us but one who is like our better selves -- not someone who plays to our fears and prejudices but someone who can embody our virtuous aspirations.
Indeed. As I argue in The Good Life: Aspiration, Dignity, and the Anthropology of Wellbeing, we aspire to be certain sorts of people -- a key part of our identity is not just who we are, but who we want to be. Our aspirations reflect certain sorts of values, what matters most to us in the big scheme of things. These aspirations, and our better selves, can be undermined by short-term gains and hedonic pleasures. And so we need leaders to remind us of our better selves and guide us down the often more arduous path of long-term personal and collective fulfillment.
For these same reasons, we also need rules to hep us be our better selves. A recent RadioLab episode (Nazi Summer Camp) looked at how the U.S. treated the 500,000 or so German and Japanese POWs in U.S. camps. It turns out we treated them exceedingly well, fully following the letter and spirit of the Geneva Convention, even when we saw that the Japanese and Germans were not so scrupulous in their adherence. Significantly, we treated the U.S. citizens of Japanese descent much worse at the internment camps. As U.S. citizens, paradoxically, there were no international rules to govern their treatment, and the country showed it worse side. Similar examples of how rules can help us be the sort of people we say we want to be can be found in Lynn Stout's excellent book Cultivating Conscience and in my book The Good Life.
Indeed. As I argue in The Good Life: Aspiration, Dignity, and the Anthropology of Wellbeing, we aspire to be certain sorts of people -- a key part of our identity is not just who we are, but who we want to be. Our aspirations reflect certain sorts of values, what matters most to us in the big scheme of things. These aspirations, and our better selves, can be undermined by short-term gains and hedonic pleasures. And so we need leaders to remind us of our better selves and guide us down the often more arduous path of long-term personal and collective fulfillment.
For these same reasons, we also need rules to hep us be our better selves. A recent RadioLab episode (Nazi Summer Camp) looked at how the U.S. treated the 500,000 or so German and Japanese POWs in U.S. camps. It turns out we treated them exceedingly well, fully following the letter and spirit of the Geneva Convention, even when we saw that the Japanese and Germans were not so scrupulous in their adherence. Significantly, we treated the U.S. citizens of Japanese descent much worse at the internment camps. As U.S. citizens, paradoxically, there were no international rules to govern their treatment, and the country showed it worse side. Similar examples of how rules can help us be the sort of people we say we want to be can be found in Lynn Stout's excellent book Cultivating Conscience and in my book The Good Life.
Subscribe to:
Comments (Atom)



